Peptic Ulcer Disease | Surgery | Bailey learned with Dr. Sandeep | PW MedEd
PW MedEd
Overview
This video explains peptic ulcer disease, focusing on its definition, causes, and the differences between gastric and duodenal ulcers. It clarifies that 'peptic' refers to the digestive enzymes like pepsin and hydrochloric acid, not just pepsin itself. The primary cause is identified as an imbalance between acid production and mucosal defense, often exacerbated by H. pylori infection. The video details the distinct pathophysiological mechanisms for ulcers in the stomach versus the duodenum, highlighting the role of metaplasia in the latter. It also contrasts the symptoms, risk factors, and potential complications of gastric and duodenal ulcers, emphasizing the importance of diagnosis and management.
Save this permanently with flashcards, quizzes, and AI chat
Chapters
- Peptic ulcer disease involves a 'breach in the continuity of epithelium or mucous membrane' with tissue death.
- The term 'peptic' is a misnomer; while pepsin is involved, the primary culprit is excessive hydrochloric acid (HCl) concentration.
- The disease arises from an imbalance between aggressive factors (like excess HCl) and protective mucosal defenses.
- Common sites include the first part of the duodenum (D1), the stomach (especially the lesser curvature's angularis incisura), the lower esophagus with gastric mucosa, and Meckel's diverticulum.
- Helicobacter pylori (H. pylori) is the most common cause of peptic ulcer disease.
- H. pylori produces urease, which converts urea to ammonia, a strong alkali.
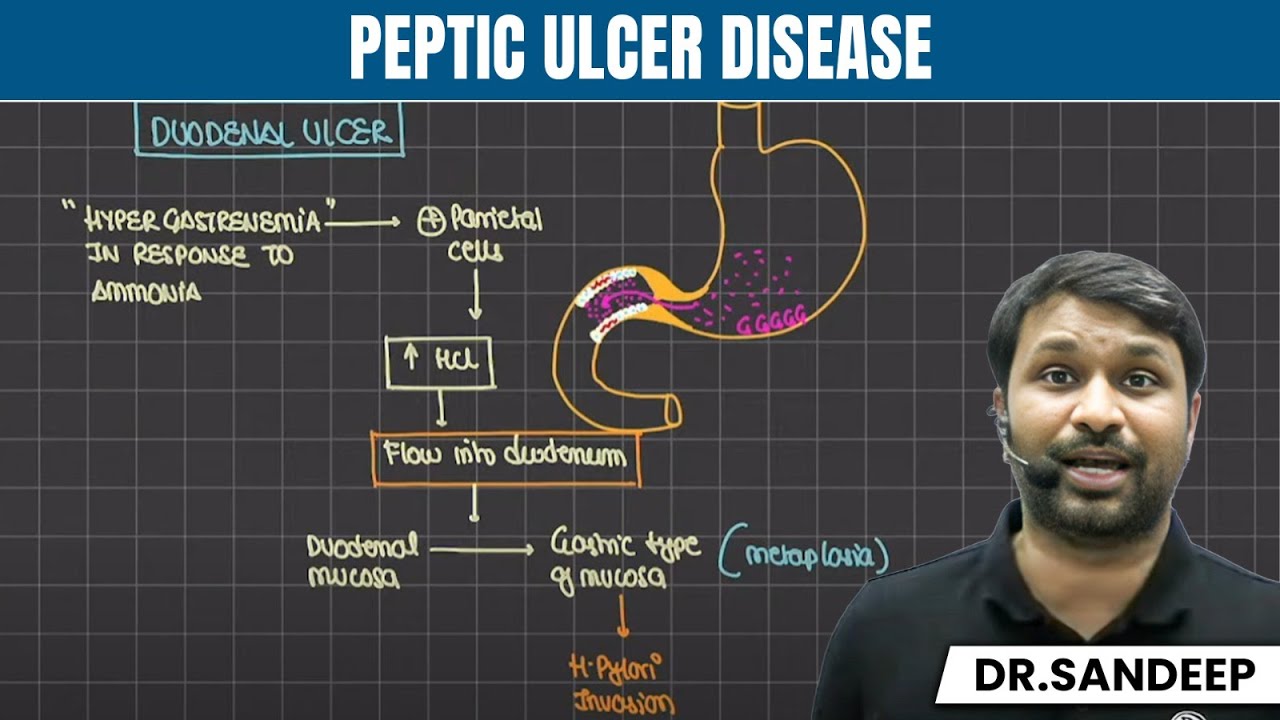
- Ammonia stimulates G cells in the stomach's antrum to produce more gastrin, leading to hypergastrinemia.
- Hypergastrinemia increases parietal cell stimulation, resulting in excessive hydrochloric acid secretion.
- Ammonia also causes inflammation and neutralizes acid, allowing H. pylori to proliferate submucosally and produce cytotoxins (CagA, VacA) that damage the mucosa.
- Duodenal ulcers occur because excessive HCl from the stomach overwhelms the duodenum's protective mechanisms.
- The duodenum undergoes metaplasia, transforming its lining into gastric-type mucosa to better tolerate acid.
- This metaplastic (gastric-type) mucosa in the duodenum then allows H. pylori to colonize and cause inflammation and ulceration.
- The process involves hypergastrinemia, increased HCl production, and subsequent damage to the duodenal lining.
- Other risk factors include smoking, NSAID (non-steroidal anti-inflammatory drug) use, and steroid use.
- Stress can lead to 'stress ulcers,' with specific types like Curling's ulcers (from burns) and Cushing's ulcers (from head injury).
- Endocrine causes include gastrin-producing tumors (Zollinger-Ellison syndrome), often associated with hyperparathyroidism.
- Gastric ulcers are more commonly associated with malignancy (cancerous ulcers) than duodenal ulcers, necessitating biopsy.
- Duodenal ulcers typically occur in a hyperacidic environment and are associated with increased appetite and weight gain.
- Gastric ulcers can form in a normal or hypoacidic environment, often leading to decreased appetite, weight loss, and immediate pain after eating.
- Pain in duodenal ulcers appears 2-3 hours after meals, while gastric ulcer pain is often immediate upon food ingestion.
- Obstruction is more common in duodenal ulcers, whereas bleeding is more frequent in gastric ulcers.
- Perforation is more common in duodenal ulcers, while gastric ulcers are more likely to be malignant.
Key takeaways
- Peptic ulcer disease is caused by an imbalance between acid/enzyme secretion and mucosal defense, with H. pylori being the primary infectious agent.
- H. pylori's urease enzyme produces ammonia, which stimulates acid production and directly damages the gastric mucosa.
- Duodenal ulcers develop when excess stomach acid causes metaplasia in the duodenum, creating a susceptible environment for H. pylori.
- Gastric ulcers are more commonly associated with malignancy and bleeding, while duodenal ulcers are more prone to perforation.
- Symptoms like pain timing relative to meals, appetite changes, and weight trends can help distinguish between gastric and duodenal ulcers.
- NSAIDs, smoking, steroids, and specific endocrine disorders are significant risk factors for peptic ulcer disease.
- Upper endoscopy with biopsy is the gold standard for diagnosing peptic ulcers, especially to rule out malignancy in gastric ulcers.
Key terms
Test your understanding
- What is the primary mechanism by which H. pylori contributes to the development of peptic ulcers?
- How does metaplasia in the duodenum facilitate the formation of duodenal ulcers?
- What are the key differences in pain presentation and appetite between gastric and duodenal ulcers?
- Why is a biopsy crucial when diagnosing gastric ulcers, and what is it primarily looking for?
- Explain the role of gastrin in the pathophysiology of peptic ulcer disease.